
Anatomy
Anatomically, the two ventricles (atria) are separated from each other by a septum. In the case of a sinus venosus defect, there is a connection between the left and right atrium through an interruption in this septum.
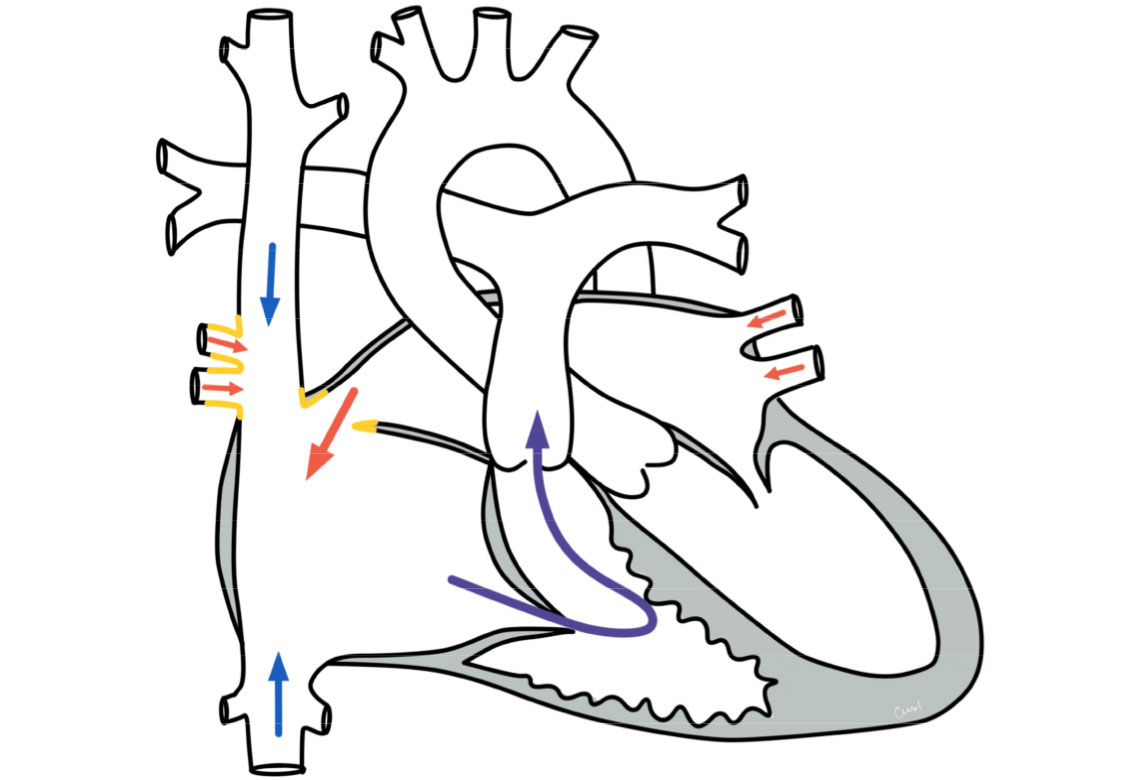
The defect is usually located at the top of the atrial septum near the junction of the superior vena cava. If the right-sided pulmonary veins also open into the superior vena cava or the right atrium, this is referred to as a partial pulmonary vein defect.
Physiology and hemodynamics
Depending on the size of the connection, more or less blood flows through the defect. As there is a slightly higher pressure in the left atrium, blood flows through the defect from the left into the right atrium (left-to-right shunt), from there into the right ventricle and then into the pulmonary vessels. This can lead to a strain on the right heart and to an over-perfusion of the lungs. In the case of pulmonary vein malformation, the blood from the incorrectly opening pulmonary veins also flows into the right atrium.
Unlike a ventricular septal defect, however, an atrial septal defect usually does not pose a risk of pulmonary hypertension, as the pressure in the two atria is significantly lower than in the main chambers. Therefore, although an atrial septal defect increases the blood flow to the lungs, there is no significant pressure load.
Therapy for a sinus venosus defect (with or without pulmonary vein malformation)
Conservative
The urgency of treatment depends on the size of the defect or the amount of blood that has been diverted and therefore on the effects on the circulation (hemodynamic relevance). This heart defect often does not lead to any relevant stress in the first few years of life, so that treatment is often carried out in pre-school age. If the heart defect is only recognized later, surgical treatment can usually be planned. In some cases, drug therapy for cardiac stress (heart failure) is necessary.
Surgery
The definitive therapy is surgery. Imaging diagnostics (magnetic resonance imaging, computer tomography, cardiac echo) are usually carried out beforehand to plan the surgical procedure.
The surgical closure is performed using a heart-lung machine, with either an approach from the front through the chest or from an angle with a small incision (MIS technique). The defect is closed with a patch made of pericardial material or other tissue (synthetic or biomaterial). In the case of an existing pulmonary vein defect, the pulmonary veins are diverted through the patch into the left atrium. After the operation, the patient is treated briefly in the intensive care unit before returning to the cardiology follow-up ward.
Prognosis for a sinus venosus defect
Further course
After closure of a sinus venosus defect, children or adults are heart-healthy. After timely therapeutic closure, normal physical capacity and an unimpaired lifestyle can be expected.
In patients with pulmonary vein defects, constrictions in the area of the bypassed pulmonary veins or the superior vena cava may occur in the further course, which occasionally require further treatment (e.g. by means of cardiac catheterization).