
Anatomy
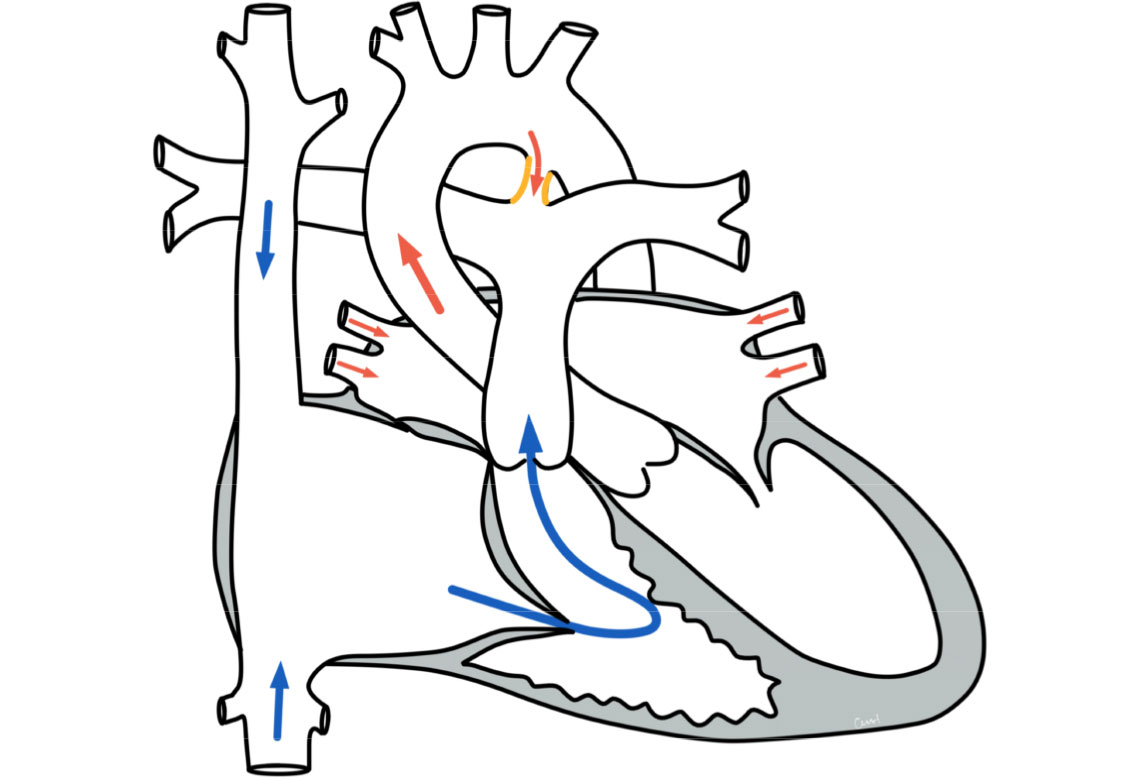
Anatomically, the ductus arteriosus serves the unborn child as a normal and necessary short-circuit connection between the pulmonary artery and the aorta in order to carry the blood past the not yet working lungs. In the first hours and days after birth, the ductus closes as part of the circulatory transition. If this closure does not take place, it is referred to as an open or persistent ductus arteriosus. This closure is more common in premature babies.
As the pressure conditions in the heart chambers and in the large vessels change after birth, the blood then flows through the remaining connection from the aorta into the pulmonary artery.
Physiology and hemodynamics
Depending on the size of the ductus, more or less blood flows through this connection into the lungs. This increased volume of blood then flows out of the lungs to the left atrium and into the left ventricle. Medium and large connections lead to an overload on the left side of the heart. This additional volume load leads to an enlargement of the left atrium and left ventricle.
A very large ductus arteriosus leads to a pressure equalization between the aorta and pulmonary artery. In the long term, the increased pressure in the pulmonary vessels leads to vascular changes, as their wall structure is not designed for such a pressure load. These changes cannot be reversed. This condition is referred to as fixed pulmonary hypertension.
Therapy for a PDA
Conservative
The time of therapy depends on the size of the ductus and thus on the effects on the circulation (hemodynamic relevance). In premature babies, closure can often be achieved in the first few days or weeks with drug therapy.
Surgery and interventional
Interventional closure is the preferred treatment option, except for very small premature babies. This involves using a cardiac catheter to position a small umbrella or coil in the ductus through a vascular access (sheath) inserted into the inguinal vessels so that the ductus is closed. After 3-6 months, the umbrella or coil is completely ingrown.
Surgical intervention is the treatment option of choice for very small premature babies in whom cardiac catheterization is not possible due to their body size. The operation is usually performed without the use of a heart-lung machine. Access is gained via a small access between the ribs on the left side of the chest. The ductus is cut off with a clip and severed.
Prognosis for a PDA
Further course
After spontaneous closure or timely therapeutic closure, the patient can be expected to have a normal physical capacity and an unimpaired lifestyle.