
Description
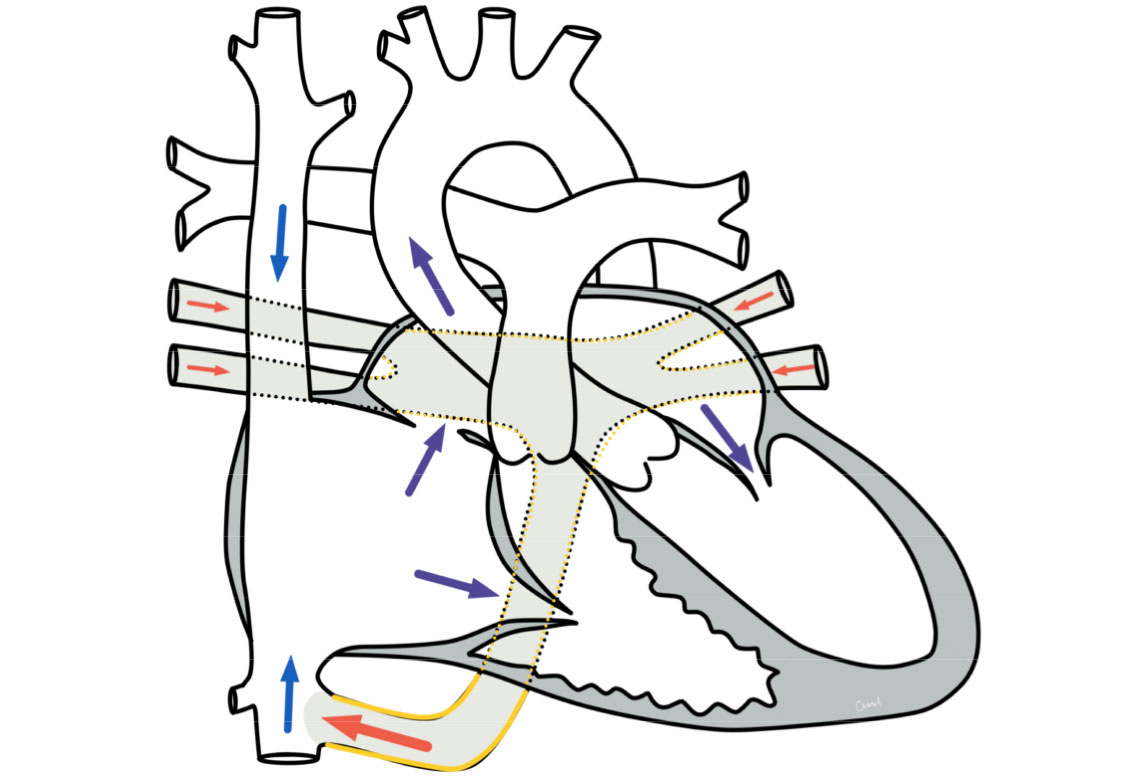
In the case of a total or complete pulmonary vein malperfusion, the oxygen-rich blood from the lungs does not reach the left atrium via the pulmonary veins, but (directly or via detours) reaches the right atrium.
If the detour leads via the superior vena cava, it is referred to as the supracardiac type, if it leads via the inferior vena cava, it is referred to as the infracardiac type (see adjacent drawing). If the collecting vessel of the pulmonary veins opens directly into the right atrium, it is a cardiac type (see also variants).
This serious heart defect (vitium) is very rare and belongs to the group of cyanotic vitias in which the blood of the systemic and pulmonary circulation is mixed, resulting in a bluish skin coloration.
Physiology and hemodynamics
Due to the confluence of the pulmonary veins with the right atrium, oxygen-rich blood from the lungs and oxygen-poor blood from the veins of the systemic circulation mix in the right atrium. This mixed blood is then pumped back into the lungs via the right ventricle on the one hand and into the left atrium via a defect in the atrial septum on the other (obligatory right-left shunt via a defect in the atrial septum). The blood flows from the left atrium into the left ventricle. This pumps the mixed blood into the systemic circulation. As a result, the body is supplied with deoxygenated blood, which causes cyanosis (bluish coloration of the skin).
The affected babies are cyanotic immediately after birth. The blue coloration is particularly visible on the tongue, lips, tips of fingers and toes.
In some children, the outflow from the pulmonary veins is obstructed. This leads to a congestion of blood in the lungs, which makes the X-ray image less transparent ("white lung").
Variants of total pulmonary vein malformation
Supracardiac, cardiac and infracardiac type
The blood from the lungs always enters the right atrium instead of the left atrium in total pulmonary vein malperfusion. If there is a collecting vessel that connects to the superior vena cava above the heart (usually via a drainage into the anonymous vein), this is referred to as the supracardiac type. If the blood flows from the lungs directly into the right atrium, it is referred to as the cardiac type of total pulmonary vein malformation. If the blood enters the inferior vena cava via a collecting vessel (usually in the immediate vicinity of the liver) below the heart, this is referred to as the infracardiac type.
Download supracardiac type of pulmonary vein malformation (PDF) Download cardiac type of pulmonary vein malformation (PDF) Download infracardiac type of pulmonary vein malformation (PDF)
Treatment of a total pulmonary vein malformation
Surgical and interventional therapy
The aim of the therapy is to correct the heart defect. In most cases, this is only possible through surgery. The operation is usually performed in the neonatal period or early infancy and must be carried out with the aid of a heart-lung machine. The pulmonary veins are correctly connected to the left atrium, the vessels of the existing bypass and the defect at atrial level are closed.
If there is an obstruction to the outflow from the lungs, emergency surgery is necessary. Sometimes interventional palliation (improvement) with a cardiac catheterization procedure is also necessary first, whereby any existing narrowing of the collecting vessel of the pulmonary veins must be removed or the connection between the two atria must be widened if it is too narrow or restrictive.
The pulmonary veins are a sensitive tissue and therefore constrictions in the area of the pulmonary veins are also likely to occur following the procedure.
Initial stabilization
If the outflow of blood from the lungs is obstructed, the affected babies are often very ill and this is an emergency that requires immediate care. Occasionally, these babies also need to be stabilized with a circulatory support system (ECMO).
Prognosis of a total pulmonary vein malformation
Further course
Surgery for a total pulmonary vein malformation corrects the heart defect. The postoperative course is essentially determined by the condition of the babies before the operation and is often more severe in very sick children with an obstruction in the area of the pulmonary veins than in stable newborns.
The affected children are generally free of symptoms after the operation. In some children, constrictions in the area of the pulmonary veins occasionally require further treatment. Cardiac arrhythmias also occasionally occur as a result of this heart defect, but these do not always require treatment.
After successful correction, life expectancy is probably comparable to that of the normal population, and everyday life should also be possible without restrictions.