
Description
Transposition of the great arteries or vessels (TGA) is one of the most common congenital heart defects, accounting for around 2-3% of cases. This heart defect (vitium) belongs to the group of cyanotic vitia, in which the blood of the systemic and pulmonary circulation is mixed.
In about 25% of cases, TGA is accompanied by other cardiac malformations (ventricular septal defect, narrowing of the pulmonary or aortic artery, anomalies in the course of the aorta, malformation of the coronary arteries).
Anatomy
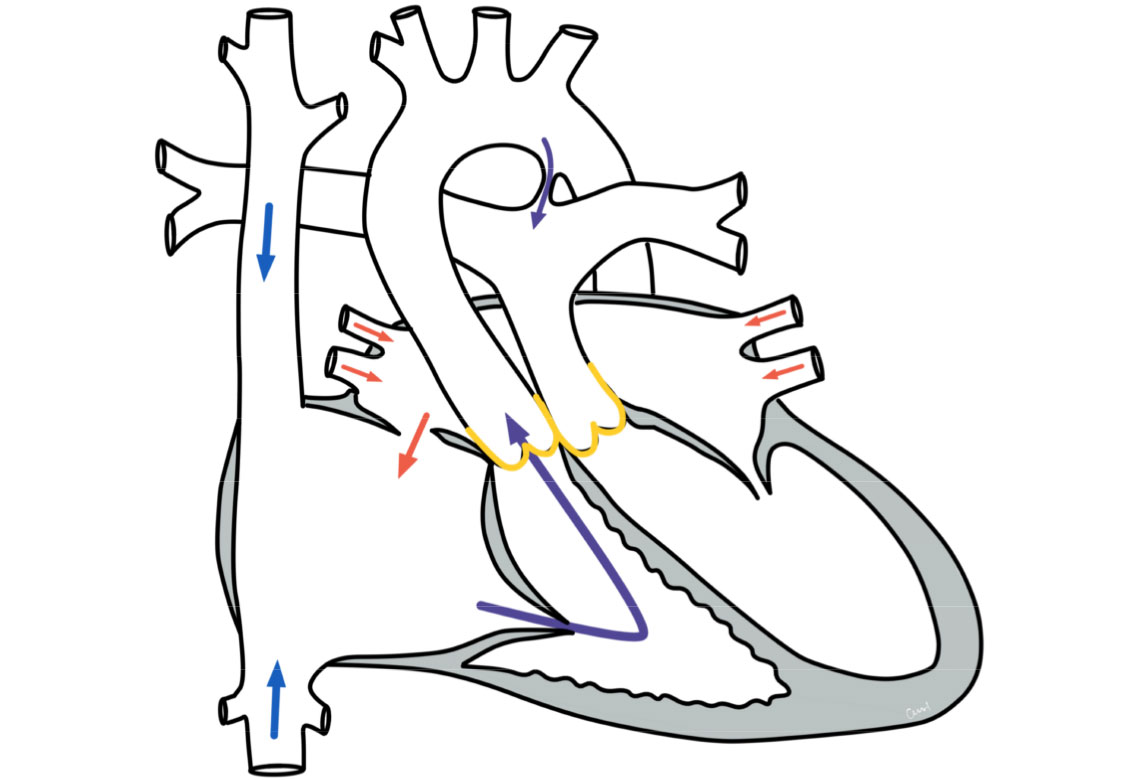
Transposition of the great arteries occurs when there is an interchanged exit of the pulmonary and coronary arteries from the ventricles. The aorta does not originate from the left ventricle as in healthy hearts, but from the right ventricle, while the pulmonary artery originates from the left ventricle. As a result, the two circulatory systems (pulmonary and systemic circulation) are decoupled from each other (connected in parallel) and not - as is normally the case - connected in series.
Physiology and hemodynamics
Due to the parallel circuits, the deoxygenated blood that arrives in the right side of the heart returns to the body via the aorta. The oxygen-rich blood that reaches the left side of the heart from the lungs is pumped back into the lungs via the pulmonary artery.
The affected babies are viable due to short-circuit connections that already existed in the womb - if these connections are closed, survival is not possible. The connections consist of a hole in the atrial septum (foramen ovale/atrial septal defect/ASD) and a vascular connection between the aorta and pulmonary artery (ductus botalli/PDA). During the fetal period, this connection serves as a bypass circuit for the lungs. A few days after birth, the PDA usually closes.
Due to these connections, there is a mixing of the two blood circulations (body and lung circulation). The body can be supplied with at least some oxygen-rich blood.
The affected babies show cyanosis (bluish skin coloration). This is particularly visible on the tongue, lips, tips of fingers and toes. The symptoms appear shortly after birth. In addition, there is often a weakness to drink, listlessness and possibly life-threatening shock. They are caused by the slowly closing short-circuit connections (foramen ovale and ductus botalli). As a result, the two circulatory systems become increasingly separated and the organs are supplied with less and less oxygen.
Treatment of transposition of the great arteries
Stabilization after birth
In the treatment of TGA, emergency measures must first be taken to keep the circulatory connections open. This includes keeping the slowly closing ductus botalli open with medication. This can improve blood mixing at the level of the large vessels.
Occasionally it is also necessary to enlarge the defect at the atrial level using a balloon catheter (Rashkind maneuver; balloon atrioseptostomy). This improves the mixing of the blood at the level of the atria. Long-term conservative therapy is not advisable. After stabilization, surgical correction is usually required in the first few days of life.
Surgery
Primary corrective surgery is then performed a few days apart and must be carried out with the aid of a heart-lung machine. The two large vessels above the heart valves are separated and repositioned (so-called arterial switch operation, ASO). It is also necessary to separate the coronary vessels from the aorta, mobilize them and sew them back into the repositioned aorta.
Concomitant malformations of the heart, particularly narrowed branches of the vessels or malformations of the coronary arteries can make the operation more difficult or, in rare cases, impossible. Other surgical procedures must then be used.
Prognosis of transposition of the great vessels
Further course
Surgical correction of the TGA is one of the standardized surgical procedures. The chances of success are very good. The postoperative course is generally uncomplicated.
In the long-term course, there is an increased risk of constrictions in the area of the sutures (anastomoses) of the transposed vessels. These narrowings are usually insignificant. For some patients, however, further interventions are necessary in the course of their lives.
After successful correction, life expectancy is comparable to that of the normal population, and patients should also be able to lead an unrestricted everyday life.