The Breast Center of the MHH
Dr. med. Elna Kühnle
The Breast Center at Hannover Medical School (MHH) is the central institution for questions relating to the diagnosis and treatment of breast diseases.
Breast cancer is of particular importance here. We offer women and men with breast cancer a holistic care concept whose high level of professional competence has been tested and certified by independent experts in accordance with the requirements of the German Cancer Society, the German Society for Senology and DIN EN ISO 9001.
Contents
- Dates | Registration
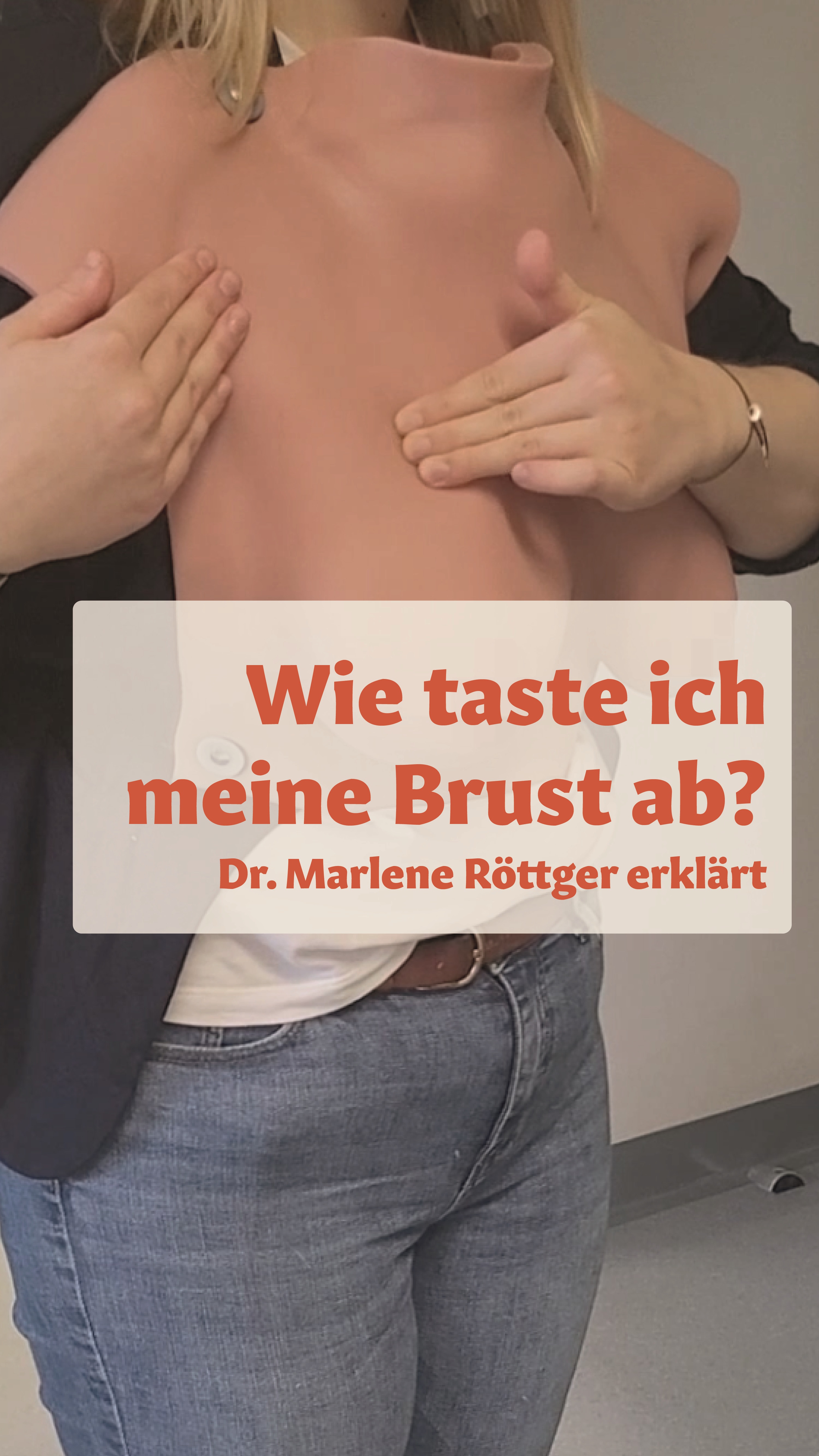
- Video: How to scan my breast
- Our area of responsibility
- Our services
- Good to know
- Supporting offers
Our area of responsibility
At our Breast Center,we care for patients who have been diagnosed with breast cancer for the first time as well as those who have suffered a recurrence or have metastatic disease. We see it as our task as a university hospital to offer them the best possible surgical and drug therapy at all times, which corresponds to the latest scientific findings and to create an individualized treatment concept for each patient.
We see it as our task as a university hospital to offer our patients the best possible surgical and drug therapy at all times, which corresponds to the latest scientific findings and to create an individualized treatment concept for each patient.
The interdisciplinary structure of the Hannover Medical School (MHH) - everything under one roof - and the close cooperation enable our patients to be referred directly to colleagues in radiotherapy, thoracic surgery, plastic surgery or internal medicine.

Our holistic approach also includes supporting measures. In addition to the connection to gynecological psychosomatics and psycho-oncology, we also provide nutritional medical support and traditional Chinese medicine (TCM) therapy options if required.
Above all, we appeal to your self-care, self-examination and early detection.
Services
Early detection of breast cancer can often mean gentler treatment and improve the chances of recovery. In many cases, small tumors detected at an early stage can be treated with breast-conserving surgery. Based on the histological examination of the tissue sample (punch biopsy) by the pathologists, a targeted and individualized therapy can already be determined for most patients.
Mammography screening
All women between the ages of 50 and 69 receive an invitation to a free mammogram every two years as part of cancer screening. Mammography screening in Hanover is organized by the Central Office of the Association of Statutory Health Insurance Physicians of Lower Saxony.
Familial breast and ovarian cancer
The MHH Breast Center is part of the German Consortium for Familial Breast and Ovarian Cancer in Germany. In 5 - 10% of all breast cancer cases, the disease is hereditary. A very young age of onset, the occurrence of breast and ovarian cancer in several members of the maternal and paternal line or the occurrence of breast cancer on both sides can be indications of a genetic cause.
If there is a certain risk constellation, genetic testing can be carried out using a blood sample in the Department of Human Genetics at the MHH.
- Mammography
Mammography is an indispensable component of breast diagnostics. This X-ray examination can be used to detect lumps in the breast as well as conspicuous calcifications in the breast. In special cases, for example when patients have very dense glandular tissue, we can take and evaluate additional tomographic images of the breast (tomosynthesis) or perform an MRI. - Ultrasound
In addition to mammography, an ultrasound examination (high-resolution sonography) is carried out. This examination procedure can provide additional information on the extent and location of the findings. Ultrasound often provides better results, particularly in women with very dense glandular tissue. As a rule, a combination of mammography and ultrasound is recommended to clarify tumors. - Magnetic resonance imaging (MRI)
An MRI of the breast can also be carried out for special questions or in intensified early detection/follow-up care. This very special examination can provide information about the presence of multiple tumor foci or tumor foci hidden by mammography and sonography. - Tissue biopsy
If the patient has a palpable lump or a finding is visible on ultrasound, a tissue sample can be taken from the lump on an outpatient basis with a thin needle under local anesthesia for a histological examination. If the mammogram reveals conspicuous microcalcifications, for example, a sample can be taken under X-ray. The result is usually available within five working days. For subsequent control of the biopsy area, the physician can place a tiny titanium clip on the sampling site during the tissue removal. Depending on the results of the histological examination, the findings are discussed in detail with all experts in the tumor conference. Subsequently, the patient will usually be consulted about the further procedure approximately one week later. We ask the patient to remember to discontinue all blood-thinning medication one week before a planned tissue sample is taken after consulting her family physician or gynecologist - Staging (spread diagnostics)
If there is an increased risk of the tumor spreading (metastases), staging is carried out in accordance with the guidelines. The liver and lungs are examined using computer tomography (CT) and a bone scintigraphy is carried out to clarify the bones.
Close cooperation between surgeons and oncologists, pathologists, radiologists and radiotherapists is aprerequisite for the optimal planning and implementation of breast cancer treatment. Today, the procedure is highly individualized and takes into account the needs of the individual patient, the results of the physical examination and imaging diagnostics (mammography, sonography, MRI, X-ray, scintigraphy) and the results of the histological examination (histology).
At the first appointment at our Breast Center, the attending physician will discuss your medical history, your current illness and the possible examination steps in detail with the patient. This is followed by a palpation examination as well as an ultrasound and, if necessary, a mammography examination of the breast and lymph drainage channels. Further examinations may be carried out if specific questions arise:
The therapeutic procedure with regard to the disease is coordinated for the patients in the tumor conference, an interdisciplinary group of specialists. Specialists from the fields of surgical and oncological gynecology, internal oncology, radiology, radiotherapy, nuclear medicine and pathology discuss the diagnosis and individual treatment of patients on a weekly basis. This enables us to offer patients high-quality treatment and participation in clinical studies and to immediately incorporate the latest findings into diagnosis and treatment. The tumor conference protocol serves as the basis for a subsequent detailed information and consultation with the patient.
The three pillars of treatment for primary (non-metastatic) breast cancer consist of surgical therapy, systemic therapies and radiotherapy.
In the metastatic situation (spread to other organs), we speak of a chronic disease and systemic therapies are in the foreground in order to delay further progression of the disease. At the same time, the therapies should also aim to maintain quality of life.
Physicians in private practice are welcome to participate in the tumor conference, and patients can also be presented for joint consultation in this setting.




This might interest you
ResearchAnother focus is on the further development of the field. In the research area of the Women's Clinic, we are dedicated to basic scientific and translational issues.
StudiesWe also offer clinical studies on breast cancer.
Drug oncology | Chemotherapy outpatient clinic
In gynecological-oncological treatment, we now have a range of modern therapeutic procedures at our disposal. In addition to surgical therapy, drug therapy (e.g. chemotherapy, targeted therapy or immunotherapy) has also become very important.
